Tubal Ligation
- Description
- Faq's
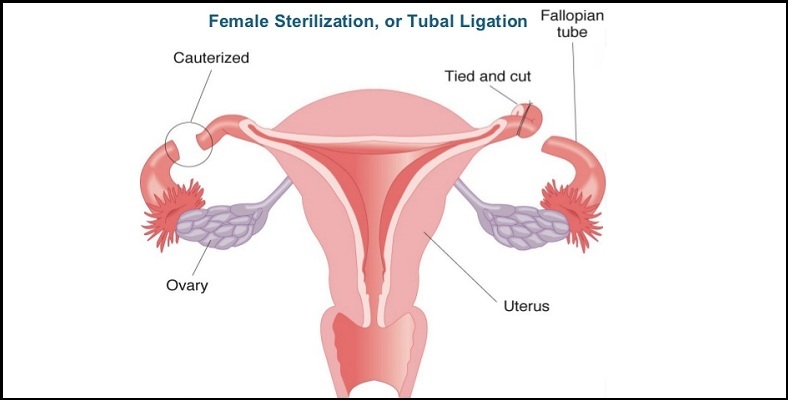
Tubal ligation, often referred to as "having your tubes tied," is a surgical procedure in which a woman's fallopian tubes are blocked, tied, or cut. Tubal implants , such as Essure, are small metal springs that are placed in each fallopian tube in a nonsurgical procedure (no cutting is involved). Over time, scar tissue grows around each implant and permanently blocks the tubes. Either procedure stops eggs from traveling from the ovaries into the fallopian tubes, where the egg is normally fertilized by a sperm.
Tubal ligation and tubal implants are considered to be permanent methods of birth control for women. They are usually done by a gynecologist. They may also be done by a family medicine doctor or a general surgeon.Tubal ligation method :
There are several different ways of closing the fallopian tubes, including clipping or banding them shut or cutting and stitching or burning them closed. Your surgeon will probably prefer one of these tubal ligation methods.
A tubal ligation can be done using a:- A laparoscopy or mini-lap. These are done by inserting a viewing instrument and surgical tools through two small incisions (laparoscopy) or one small incision (mini-lap) in the abdomen.
- Postpartum tubal ligation This is usually done as a mini-laparotomy after childbirth. The fallopian tubes are higher in the abdomen right after pregnancy, so the incision is made below the belly button (navel). The procedure is often done within 24 to 36 hours after the baby is delivered.
An open tubal ligation (laparotomy) is done through a larger incision in the abdomen. It may be recommended if you need abdominal surgery for other reasons (such as a cesarean section) or have had pelvic inflammatory disease (PID), endometriosis, or previous abdominal or pelvic surgery. These conditions often cause scarring or sticking together (adhesion) of tissue and organs in the abdomen. Scarring or adhesions can make one of the other types of tubal ligation more difficult and risky.
Laparoscopy is usually done with a general anesthetic. Laparotomy or mini-laparotomy can be done using general anesthesia or a regional anesthetic, also known as an epidural.Reversing a tubal ligation is possible, but it isn't highly successful. This is why tubal ligation is considered a permanent method of birth control.Tubal implant method :
Implants, such as Essure, are inserted in the fallopian tubes without surgery or general anesthesia. The procedure is done in a doctor's office, an outpatient surgery center, or a hospital, and it doesn't require an overnight stay. The implant procedure itself takes about 10 minutes.
- Before the procedure, your cervix is first opened (dilated) to reduce the risk of injury to the cervix. Your doctor will use a speculum and a dilating instrument to gradually open the cervix just before the procedure.
- For the procedure, you are positioned as you would be for a pelvic exam. Your doctor passes a thin tube (catheter) through your vagina and cervix, into the uterus, and then into a fallopian tube. The catheter is used to place an implant into a fallopian tube. An implant is then placed in the other fallopian tube the same way. You may have some menstrual-like cramps afterwards.
After the procedure, an X-ray is taken to make sure the implants are in place and the tubes are closed.
In some cases, a tubal implant can be difficult to insert. Should this happen, a second procedure is needed to completely block both tubes. For the first 3 months after insertion, you must use another method of birth control. At 3 months, dye is injected into your uterus and an X-ray is taken (hysterosalpingography) to make sure that the implants are in place and the tubes are fully blocked by scar tissue. If they are, you will no longer have to use another method of birth control.